
Carotid Stenosis
Minor surgery often enough to prevent a stroke
Following a minor stroke, more and more patients are treated surgically to prevent a major one.
Eversion TEA is a new method to remove dangerous residues in the carotid artery at the neck. It is now accepted as the most effective and secure therapy to prevent a stroke, caused by a narrowing of the carotid artery.
In Switzerland, 16.000 patients suffer a stroke each year. A fourth of them are caused by calcification and fatty residues within the carotid artery, leading to a narrowing of the vessel. When these residues (also called plaque) burst or cause a clot, they can enter the flow of blood and cause an embolism.
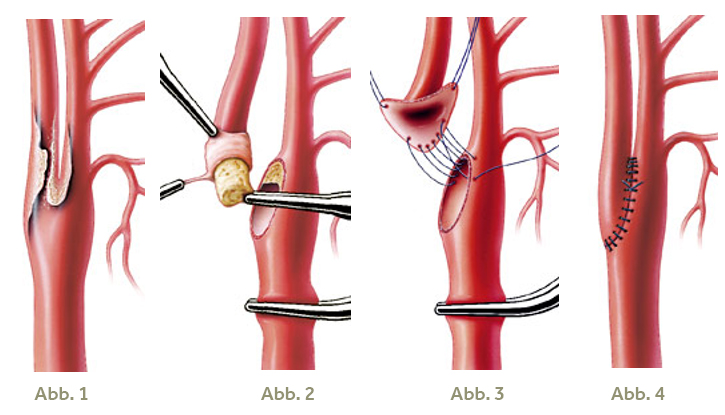
fig. 1
Carotid bifurcation with narrowing plaque, which could lead to an embolism and hence a stroke.
fig. 2
The carotid artery is disconnected. During Eversion TEA the inner branch is cut out of the bifurcation. To remove the whole plaque cylinder, the carotid wall is everted at the appropriate layer and pulled down over the cylinder.
fig. 3
With a continuous spacer seam (parachute technique), the inner branch is put back into place along the ropes of the «parachute».
fig. 4
Finishing of the reconstruction by tying the seam. The anatomical restoration of the carotid bifurcation is achieved without synthetic materials.
When is an operation recommended?
Cases of a minor stroke and a 50 percent narrowing of the carotid artery are considered neurological emergencies. These patients profit from an immediate operation, because they are otherwise likely to suffer a renewed and more severe stroke with serious neurological failures. They are the main concern of carotid surgery.
If a patient has permanent neurological failures, e.g. paralysis of the face or legs, an operation is only performed after the patient has been stabilised. In patients without symptoms, that show a narrowing of the carotid artery above 70 percent, a surgical intervention is indicated to prevent a stroke in the first place.
The aim of the operation is to remove any plaque within the artery and thus prevent the stroke. Using ultrasound, it is quite easy to judge the arterial function. Moreover, a neurologist is consulted before and after the operation.
Gentle procedure
The arteria carotis communis (or common carotid artery) splits up into two branches at the carotid bifurcation (fig.1). One of those is called the outer carotid artery (arteria carotis externa), the other the inner carotid artery (arteria carotis interna), going directly to the brain. During Eversion TEA, the carotid bifurcation is disconnected and the inner carotid artery is cut out of the bifurcation and mobilised. The artery is accessed using an almost horizontal cut along the lines of the lower jaw, guaranteeing an ideal cosmetic result, with a near-invisible scar. The operation can be performed with general, regional or even local anaesthesia.
The crucial step of Eversion TEA is the removal of the whole plaque cylinder in the right layer of the tissue, using a magnifying glass and microsurgical technique. The carotid wall is everted and pulled down over the cylinder, just like a rolled-up shirt sleeve (fig. 2). The healthy tissue layer separates itself from the plaque and remaining parts are removed carefully. Afterwards, the common and outer carotid arteries are also cleared of any residue.
The distal end of the everted part of the inner carotid artery is monitored carefully to maintain a stable connection with the normal inner layers of the vessel. The artery is then rolled down over an extension pin and expanded. To achieve optimal haemodynamics, the bifurcation is anatomically reconstructed. Any prolongation or kinks are corrected. In Eversion TEA, the placing of a synthetic patch is foregone, because the artery is not entirely cut open, as is the case in other procedures, and thus the danger of a narrowing, caused by the scar, is eliminated.
For the reconstruction of the carotid bifurcation, a very fine nylon thread is used (fig. 3). Before the tying of the seam, the vessels are rinsed and vented to make sure that no thrombi or air particles are carried to the brain (fig. 4).
Intra-operative neuromonitoring and angiography
Brain function is monitored at all times, during the disconnection of the carotid artery (which lasts around 20 minutes). If the patient is awake, this is done by conversation and movement test. In a narcotised patient, intra-operative electrophysiological monitoring and flux measurements are used. For quality control, an intra-operative angiography should always be performed, to adapt surgical technique if needed. Those measures are decisive to guarantee a low risk of complications.
Good results over the long term
The modern Eversion TEA technique has significant advantages and leads to a further improvement in long-term results. The correct anatomical reconstruction of the carotid bifurcation without a synthetic patch guarantees an ideal flow ratio. Moreover, the duration of the operation is reduced, leading to a shorter disconnection of the carotid artery. The stitching line, which oftentimes has lead to a renewed narrowing, is relocated to the wider are of the bifurcation and the inner artery remains without cut or seaming material.
Surgery is always only part of a therapy. It is essential to eliminate other diseases and reduce risk factors for arterial calcification (smoking, high blood pressure, diabetes, high cholesterol and obesity). This is done in close cooperation with general practitioners and internists. In the first year following surgery, two follow-up inspections are performed, after that one per year. This is done to prevent a renewed narrowing of the carotid artery.